Understanding the OCD cycle

If you’ve ever felt like your own mind has been hijacked by a thought you can't shake, you aren't alone. OCD isn't a personality quirk—it is a biological process that can feel incredibly isolating. By understanding the mechanics of the "OCD loop," you can begin to take the power back and find a path toward clinical stability.
The Anatomy of OCD
Moving Past Intrusive Thoughts
In popular culture, Obsessive-Compulsive Disorder (OCD) is often reduced to a quirk—a preference for symmetry or a drive for cleanliness. For those living with OCD, it is not a personality trait; it is a chronic, time-consuming biological loop that can derail daily productivity and exhaust life’s vital resources.
Today, we strip away the misconceptions and speak plainly about the science of your recovery. To resolve the distress caused by OCD, we must first untangle the mechanics of the "OCD Cycle" and understand how the brain’s alarm system has become mis-calibrated.
Obsessions & Compulsions
Clinical OCD is defined by a two-part cycle: obsessions and compulsions. While many people experience occasional intrusive thoughts or repetitive habits, OCD involves a level of intensity that causes significant functional impairment.
Obsessions are repetitive, unwanted intrusive thoughts, images, or urges. These are not reflections of your character or desires; they are biological "noise" that triggers intense distress or anxiety. Common obsessions include:
Contamination: Persistent fears regarding germs, chemicals, or environmental pollutants.
Responsibility/Harm: Intrusive thoughts about accidentally or intentionally hurting oneself or others.
Symmetry and Exactness: An overwhelming need for items to be aligned "just right" or for tasks to be completed in a specific, perfect order.
Scrupulosity: Excessive concern with morality, blasphemy, or religious perfection.
Compulsions are the repetitive behaviors or mental acts that an patient feels driven to perform in response to an obsession. The goal of a compulsion is to "neutralize" the anxiety or prevent a feared event. Common compulsions include:
Cleaning and Washing: Excessive handwashing or ritualized grooming.
Checking: Repeatedly verifying that doors are locked, appliances are off, or that no mistakes were made.
Repeating: Re-reading text, tapping, or repeating certain words to "undo" an intrusive thought.
Mental Rituals: Compulsive praying, counting, or reviewing past events to find "certainty."
The Biological Mechanism
Why the Loop Persists
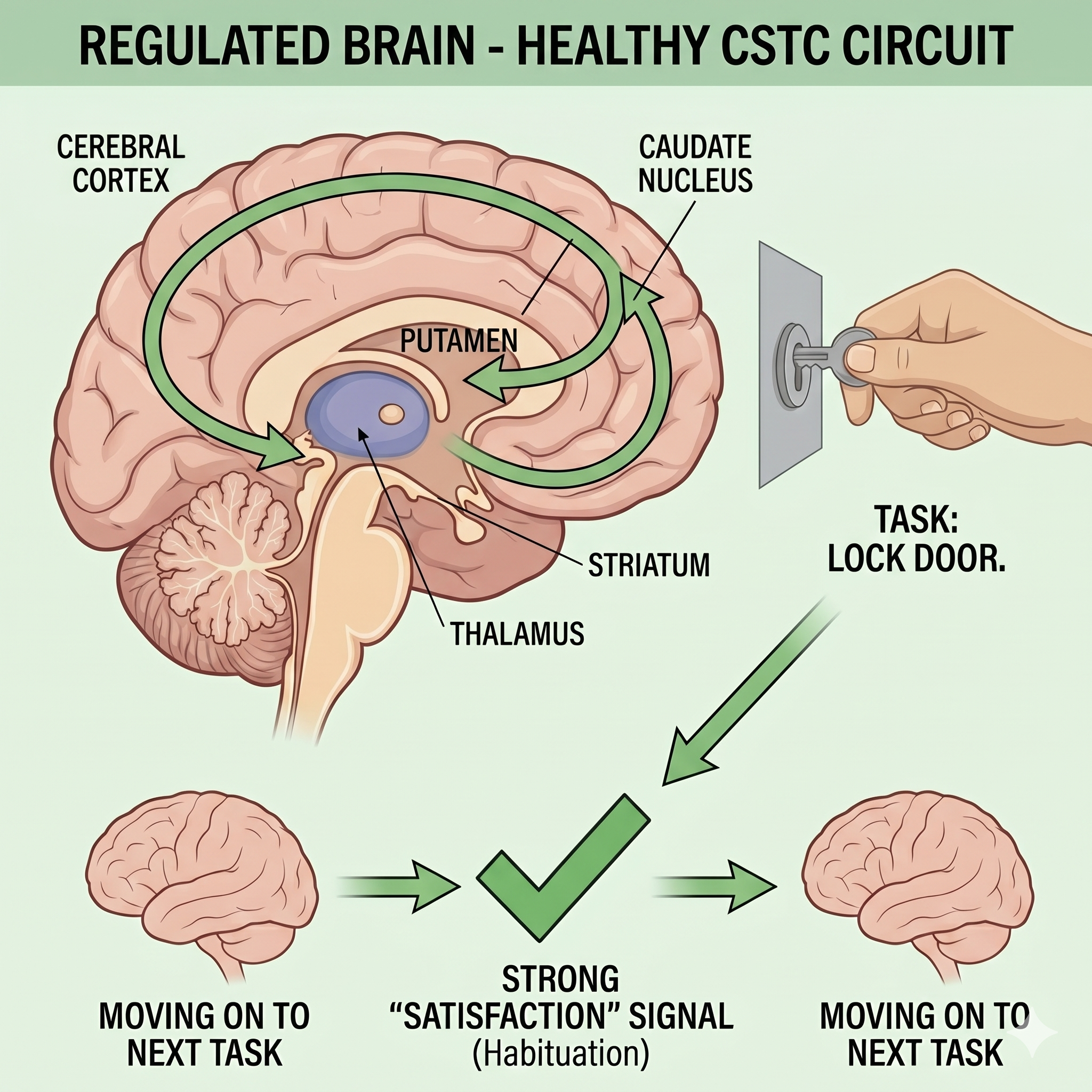
To find stability, we have to look at why the brain gets "stuck." Research indicates that OCD involves dysregulation within the cortico-striatal-thalamic-cortical (CSTC) circuit. This is the pathway in the brain responsible for habit formation and the "stop" signal for behaviors.
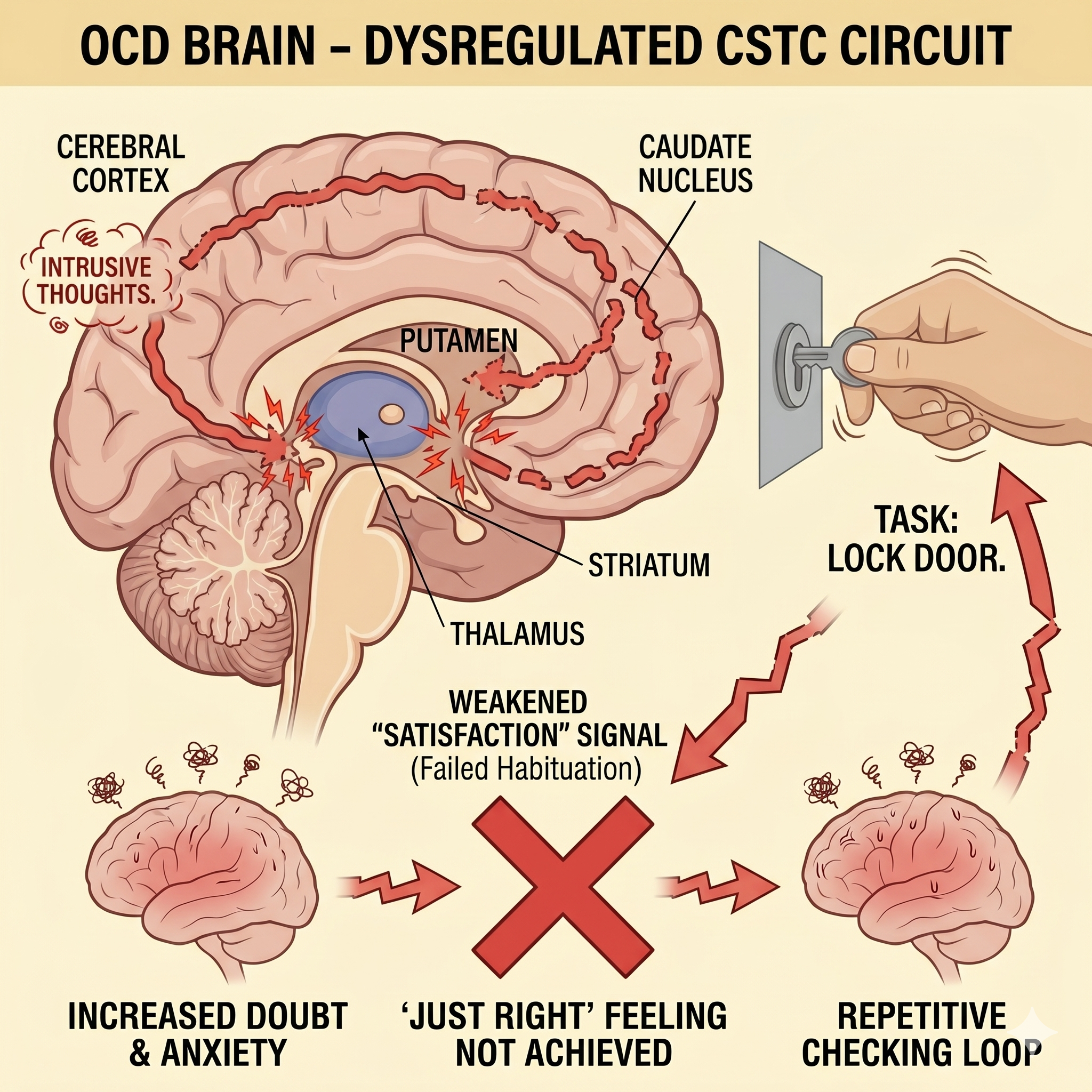
“In an OCD brain, the 'satisfaction signal' is weakened, keeping the system in a state of high alert.”
The Basal Ganglia—the part of the brain that helps filter thoughts and actions—fails to filter out the intrusive obsession. This results in a persistent feeling that something is "wrong," driving the individual to perform a compulsion to find relief. See illustration below for further details.
-
The illustration demonstrates that in OCD, this key circuit is dysregulated (marked by the starburst), causing a breakdown in communication. Specifically, the inset highlights how the Basal Ganglia fails in its crucial role as a filter, allowing intrusive, obsessive thoughts (represented by question marks and crossed-out brains) to remain unfiltered and cause distress.
This underlying biological fault directly drives the behavioral cycle shown: after a simple task like locking a door is completed, the dysregulated brain fails to generate a normal "Satisfaction" Signal, resulting instead in a Weakened "Satisfaction" Signal (warning triangle). This absence of completion leads to a persistent, nagging cognitive feeling that "Something is Wrong," which ultimately compels the individual to perform repetitive behaviors, or Compulsions, such as Persistent Checking, to gain fleeting relief.
The Trap of Temporary Relief
The danger of the OCD cycle is that compulsions actually work—but only for a moment. Performing a ritual provides a brief drop in anxiety, which reinforces the brain's belief that the compulsion was necessary for survival.
This creates a "bottom-up" loop where the compulsion feeds the obsession. Over time, the cycle requires more frequent and complex rituals to achieve the same sense of safety. This is why "just stopping" isn't a viable solution; the nervous system is reacting to a perceived existential threat that requires a clinical intervention to resolve.
The Gold Standard
Evidence-Based Treatment
Resetting this biological baseline requires a collaborative alliance and a specialized approach. At Tranquil Path Psychiatry, our integrated care focuses on the two most effective clinical tools for OCD:
1. Exposure and Response Prevention (ERP)
ERP is the most effective form of behavioral therapy for OCD. It involves carefully and systematically exposing yourself to the thoughts or situations that trigger anxiety without performing the compulsion. By resisting the urge to "neutralize" the distress, you allow your nervous system to learn that the feared outcome is not happening. This process, known as habituation, eventually weakens the OCD loop.
2. Integrated Medication Management
This is where my medical background serves us well for your care. For many patients, the physical intensity of OCD-related anxiety is so high that engaging in therapy feels impossible. Psychiatric medication, specifically Selective Serotonin Reuptake Inhibitors (SSRIs), can help regulate the neurochemistry within the CSTC circuit.
Stability: Medication "lowers the floor" of the anxiety.
Clarity: It reduces the "volume" of intrusive thoughts.
Optimization: It provides the neurological space needed for behavioral changes to take root.
Reclaiming Your Time
OCD is a demanding condition, but it is undoubtedly treatable. Recovery is not about never having an intrusive thought again; it is about building a system where those thoughts no longer have the power to dictate your actions or drain your energy.
Whether we connect in my Manalapan office or through secure telehealth, our work is centered on giving you the clarity and confidence you need to move forward and feel like yourself again.
Your Path Forward
If you are ready to move past the OCD loop and regain your stability, let’s begin with a clinical evaluation.
Frequently asked questions
-
While every case is unique, many patients begin to see a reduction in the intensity of their symptoms within 8 to 12 weeks of starting a combined approach of medication and ERP. Consistency in "not doing" the compulsions is the primary driver of success.
-
No. Perfectionism is often a personality trait that can be helpful or rewarding. OCD is a clinical disorder characterized by intrusive thoughts that cause distress and compulsions that feel mandatory. Clinical OCD usually results in a loss of time and a decrease in quality of life.
-
Absolutely. Secure, HIPAA-compliant telehealth is an excellent medium for both psychiatric evaluations and the monitoring of your medication management plan. We provide state-wide reach for all New Jersey residents.